Temporomandibular Disorders Evaluating and Management in Clinical Setting
Introduction
Not to be confused!
TMJ = Temporomandibular Joint (Joint Complex)
TMD = Temporomandibular Disorders (Diagnostic Group)
Temporomandibular Disorders earliest recordings were in ancient Egyptian times.
1900’s Disc Removals were performed, strangely enough this is still performed on occasion.
1930’s (Occulusion/ Adjusting mandibular position) this is the most popular method and is still in use despite refuting evidence.
TMD prevalence is estimated to range from 5% to 90%, this large variance is due to the difficulty to report on it’s prevalence because there is different diagnostic qualifications amongst healthcare professionals and a lack in investigative designs for studies.
Temporomandibular joint disorders can present as early as birth to 5 years of age (Birthing process can be traumatic). 6–12 years of age (Stress manifesting, contact sports, anxiety).
In Australia it is estimated that 2.5 Million adults have some form of temporomandibular disorder.
There are different ways, symptoms and variations of Temporomandibular Disorders:
24% Experience clicking, grinding, popping sounds with jaw movement
16% experience joint pain
15% Myofascial pain
10% difficulty and limitation in jaw range of movement
7% difficulty with lateral deviation of the TMJ
Mild TMD: At least 1 Symptom: 39%
Moderate TMD: At least 2 symptoms: 17.6%
Severe TMD: Three or More symptoms: 9.2%
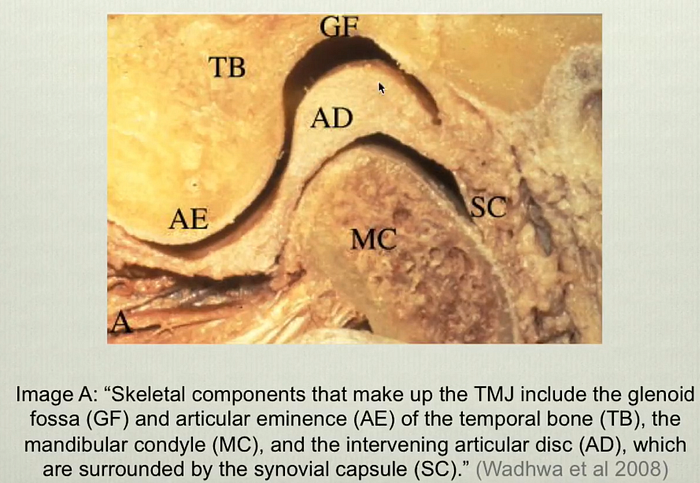
Anatomy
The jaw joints have the same anatomical components as other joints of the body.

- Bone: mandibular condyle and the glenoid fossa
- Cartilage: proximal and distal joint surfaces
- Disc: biconcave, intraarticular, divides joint into upper (discotemporal) and lower (discomandibular) spaces
- Musculature: located in the head, face, and neck; contributes to movement and stability (Boering 1979)
- Tendon: e.g. temporalis insertion on the coronoid (Benninger et al 2012)
- Other soft tissue: e.g. retrodiscal tissue (Lee et al 2009)
The details of Structures to pay attention to (In order of Most Commonly Occurring):
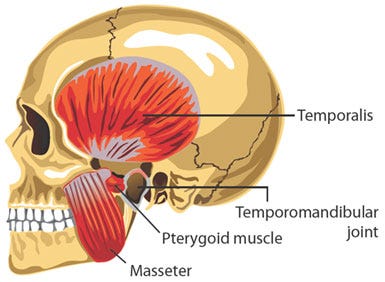
- Temporalis Muscles / Proximal Portion of Temporalis Tendons
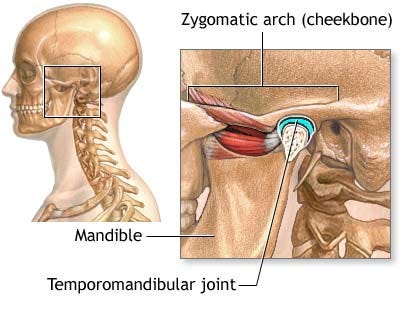
- Zygomatic Arches
- Mandibular Condyles
- Retrodiscal Spaces / Tissue
- Coronoid Processes / Distal Portion of Temporalis Tendons
- Masseter Muscles
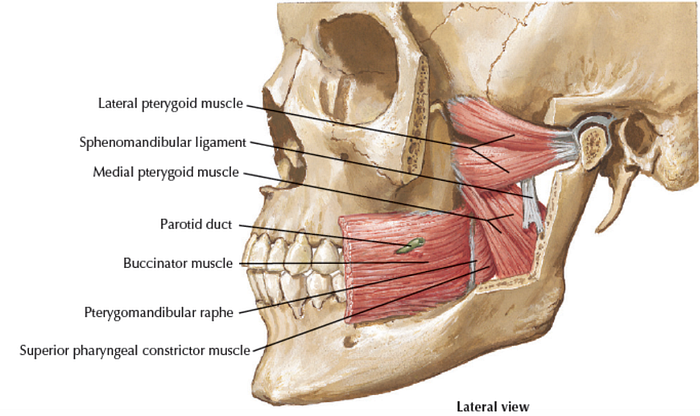
- Medial Pterygoids Muscles
- Lateral Pterygoids Muscles
Note: Knowledge and skills in assessing these structures and appreciation of the cervical spine is required to help with TMD (Always note that the cervical spine has a very close proximity to the Jaw).
Intra-Aural Muscles
Note that some of the muscles like the lateral and medial pterygoid are Intra-Aural (are only accessible from inside the jaw).
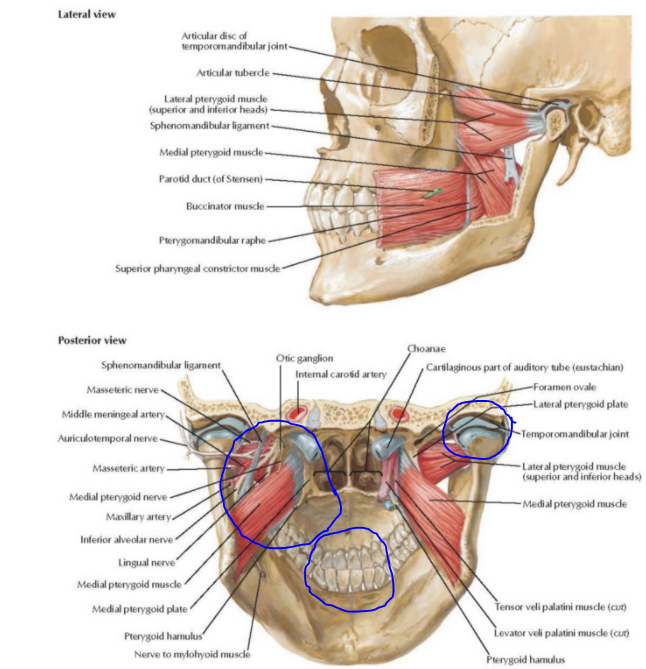
Important bony landmarks

The joint capsule & Retrodiscal Space
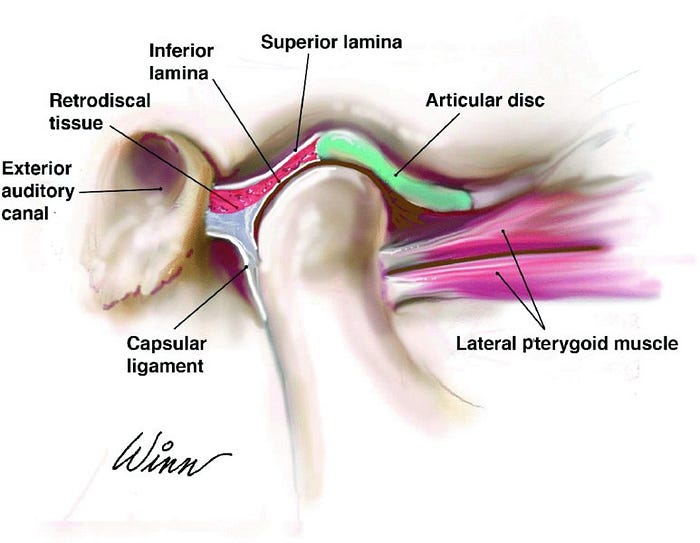
The retrodiscal tissue, connects the disc to the adjacent anatomical tissue.
Surface anatomy and the retrodiscal space (Anterior to the ear)
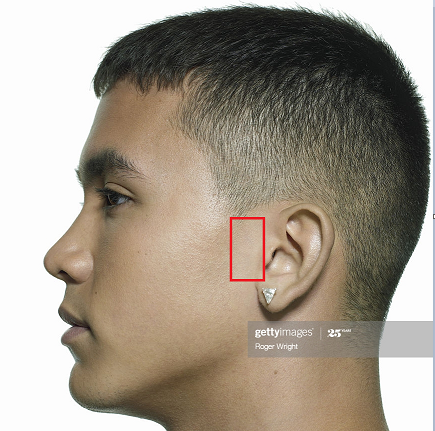

When the mouth is closed — there is a “fullness” in the retrodiscal space; jaw is in a packed/ closed position.
When the mouth is opened, there is an indentation or an appearance of a fossa, this is because when the mouth is opened — the mandibular condyle has moved forward.
During palpation, movement of the mandibular condyle should move forwards on both side. Pay attention to a lack of “fossa” felt on single side, or a lack of it bilaterally.
Pathophysiology of Temporomandibular Disorders
In the case of Temporomandibular Disorders, the joint, musculature and retrodiscal space contents can become pathological and problematic for an individual.
It is known that joint degeneration can begin as early as the age of 20. However degenerative changes on radiographic imaging are seldom correlated.
It is important to consider the onset of the following symptoms, and how each presentation of TMDs may differ.
- VAS pain of TMJ
- Tenderness on Palpation of the TMJ
- Mandibular Mobility
- Pressure Pain
However swelling in the joint (Joint Effusion) is closely related to MRI findings due to the underlying inflammatory process occurring.
Mandibular Condoyle Malformation
The mandibular condyle can undergo malformation/ defects.
Aplasia (Failure to develop and therefore function normally), this can be primary (developmental) or secondary (degeneration due to rheumatic disease, chemotherapy)
Hypoplasia (Incomplete development), primary or secondary.
Hyperplasia (Overdevelopment) which can be Hemimandibular Hyperplasia, Hemimandibular Elongation or a Combination.

Picture above shows a Right sided hemimandibular hyperplasia. There is a frontal plane asymmetry with caudal displacement of the mandible bone while the chin remains primarily in midline (Note the lack of Deviated Chin).

Picture above shows a Left sided Hemimandibular Hyperplasia. Because there is a transverse plane asymmetry with horizontal displacement of the mandible and chin (Chin not in-line with nose) away from the affected side (no caudal displacement).
Joint Restrictions of the Temporal Mandibular Joint Capsule
Restrictions in the joint capsule are very common in clinic. The few points to consider during evaluation:
Any joint going through a period of immobilization will undergo some form of capsular restriction and adhesion. Restrictions are commonly associated with a thickening of the capsule and is directly related to the length of time of immobilization.
The shortened portion of the capsule is often to blame for movement restrictions and often times adjacent joints can be affected (A tight jaw/ immobile can result in Neck articular restrictions).
When restrictions and adhesions form — the intraarticular pressure can double after just 12 weeks of immobilization.
Disc Displacement in Temporomandibular Joint
A common cause of TMD can be a result of disc structure displacement (retrodiscal tissues are also susceptible to inflammation and adhesion formation — this is important clinically), although there is very little correlation between the presence of degenerative changes of the disc and its position — it is know that frequent disc displacements can overtime create distortion/ damage/ wear & tear into the anterior ligamentous capsule.
Videos to Orientate Disc & Displacements!
Disc displacements are significant clinically, because it can be treated conservatively to speed up the natural process in allowing the jaw to open pain free. For most clients having a disc displacements can be painful in the beginning, however the “Noise” or “Clicking Sensation”, pain and function can be reduced in most cases.
Note that, it may be impossible to be rid of the clicking (However it shouldn’t be the focus of therapy if symptoms such as pain, and function returns). The focus of therapy should be on the health of the retrodiscal tissue.
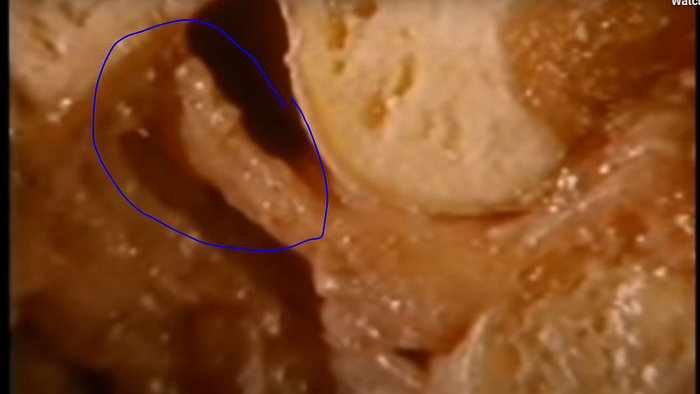
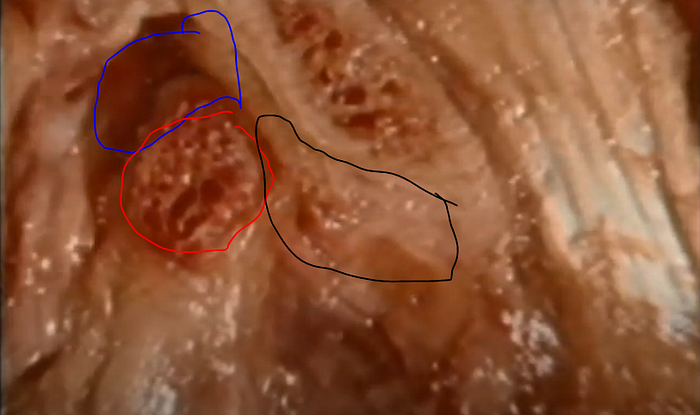
In a painful temporomandibular joint, notice how the retrodiscal tissue is misplaced and is forced to weight bear (Blue Circle)! In the pic above the disc (Black circle) has been displaced too far forwards. Here the retrodiscal tissue will undergo pressure, inflammation and is susceptible to adhesions.
Bruxism (Teeth Clenching and Grinding)
This occurs in up to 20% of the adult population and up to 66% of TMD patients report having bouts of bruxism.
Awake Bruxism — Teeth Clenching all the time.
This is a habit that can form out of stress and anxiety, clients may not be aware of it’s occurrence until it is pointed out to them.
Nocturnal Bruxism — Clenching only at night
This is an involuntary movement disorder which involves grinding of the teeth during sleep that can be audible to an observer. It can create non-restorative sleep, tooth destruction, myofascial pain, temporal headaches, divorce (marital problems due to nocturnal noise).
Pain may nor may not be present in the morning.
Temporal Headaches due to Bruxism
Temporal headaches are common due to myalgia (Dull achy sensation in muscles, tenderness, fatigue and tight sensation). In bruxism muscle pain is broad and bilateral due to the nature of the jaw activating bilaterally).
EMG readings in TMD groups shows no significant difference between normal population.
Muscular type Pain can be a result of mechanical stimulation of the tissue as prolonged clenching/ excessive use of muscles results in:
- Accumulation of Waste Products
- Vasoconstriction of Arteries & Chemical Changes in Muscular Environment
- Chemical buildup in muscle tissue of Bradykinins & prostaglandins
- Muscular type pain can also be due to Myofascial Trigger Points.
Insertional Tendinopathy in Temporomandibular Disorders
Tendinopathy can occur in the larger jaw muscles and often a confirmation of the following can be obtained via medical imaging:
- Exaggerated Dysfunctional Repair Response
- Observation of increased Fibroblasts, vascular hyperplasia, hypercellularity and disorganized collagen formation.
Temporalis Tendon (also referred to as coronoidalalgia) & Masseter tendons are the most common tendons to undergo tendinopathy & degeneration.
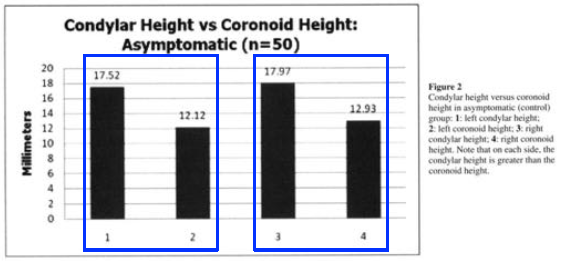
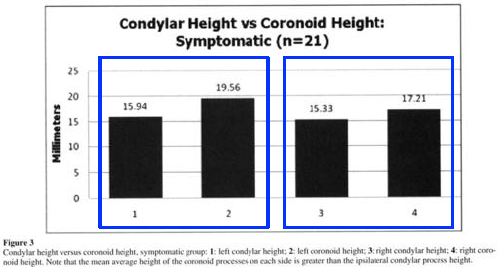
Tendinopathy in the Temporalis can last for 7.5 years or longer & can emerge due to an increase in Length of coronoid process compared to the mandibular condyle (5.4–5.8mm) length difference.
Masseter Insertional Tendinopathy
This appears in 17% of cases and results in palpable pain and tenderness found in the anterior portion of masseter origin at the zygomatic arch. This pain diminishes at the distal half side of the muscle. There is usually a history of trauma involved.
Masseter Insertional Tendinopathy Common Symptoms:
- Pain with Mastication
- Limited ROM
- Some Signs of Swelling
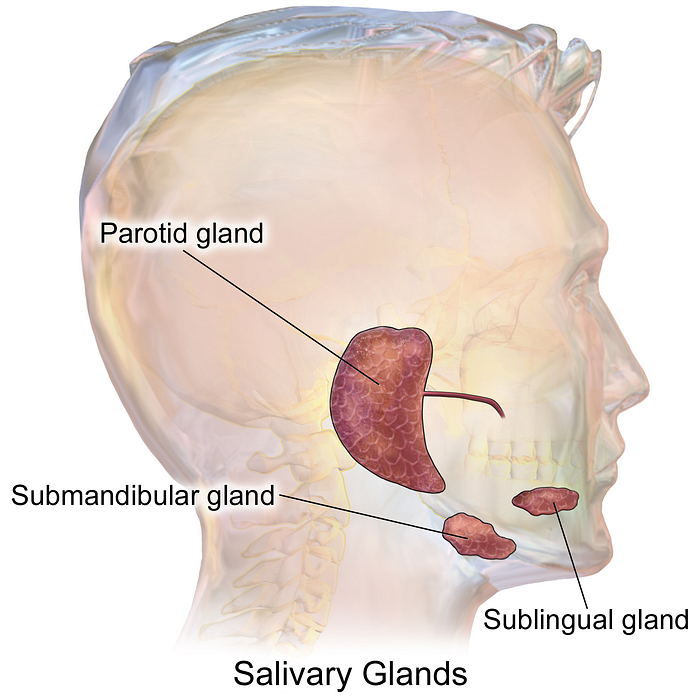
Pathoanatomy — Oral Anatomy
These are conditions that may require medical attention and interfere with the differential diagnosis of Temporo mandibular disorders.
Areas & Conditions to pay attention to:
- Parotid Glands: Lies on top of the jaw joint, can be afflicted with Sialolithiasis which is the development of calcified structures and causes blockage of ducts and salivary glands. Generally sialolithiasis will present with swelling & pain during salivation (salivary stimulus is present). Pain here does not appear when chewing or exerting force on joint — it appears primarily during the process of salivating.
- Submandibular Glands: Can also be affected with Sialolithiasis and swelling at the location.
- Tonsils: Enlarged and infections can create referred pain to the jaw joint.
- Uvula
- Soft and Hard Palates
- Teeth
- Gingivae & Frenulum of upper and lower lips
- Lymph Nodes: Swollen Lymph Nodes can create pain close to the jaw.
To Be Continued……..