On Infrasternal Angles and Respiration
What is the Infrasternal Angle (ISA)?
- The concept of Measurement of the Lower Thoracic Opening below the sternum.
- Xiphoid Process and lower ribs (False Ribs)
Knowing the ISA is handy for understanding:
- What the Non-Sternal Ribs are moving or positioning themselves in space.
- And what position the diaphragm is in during “rest”
- Identify compensatory mechanics
- Relationship to the Pelvis and Pelvic Angle (Infrapubic Angle)
Does Airflow matter for Human Movement?
It matters to breathe well —(4 P’s) our Movement Patterns, Posture, Performance, Pain are interlinked with breathing.
Models for Lung Mechanics and influence on Human Movement:
- Right & Left Lung expansion discrepancy and Lateral Flexion ability
- For Scapula Function
- For Spinal/ Dynamic Stability
- Compensatory Strategies (Different Roles of Top, Abdominal and Pelvic Region) (Top Transverse; Abdominal Frontal; Pelvis Saggital)
- Role of Abdominal Compression In Balance.
- Relationship with Pelvis Angle (Infrapublic Angle)
How do you measure the Infrastrenal Angle (ISA)?
- Find the Xiphoid Process (This forms the Apex of your Measurement)
- Measure from the side of the ribs 7–10 rib cartilage sides.
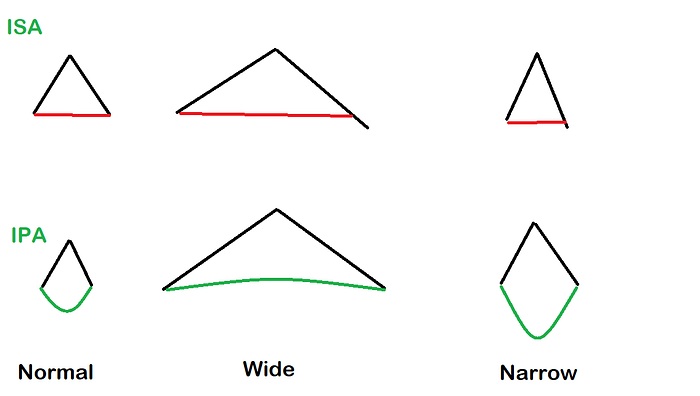
What is a normal Infrasternal Angle?
To put it simply, it is unknown what a normal infrasternal angle is. The infrasternal angle is unique to each individual and their musculoskeletal system.
What we want in our clients is to have a dynamic infrasternal angle during breathing and meaningful tasks.
This allows a person to have enough mobility in the ribs to experience a full inhalation and exhalation.
This is handy in determining what is ‘optimal’ for the ranges of motion happening in our extremities.
We want clients to be able to widen their Infrasternal Angle during Inhalation — and decrease their angle during exhalation.
It is known that individuals who are inclined towards ‘narrow’ or ‘wide’ ranges do not have normal ranges of motion in their extremities.
Testing Infrasternal Angle Variability/ Dynamic Movement
- Patient in Supine Position
- Determine the infrasternal angle
- Patient gradually flexes both shoulders until ribcage begins to “lift off” or roll superiorly towards head, this marks the point where the thorax is tipping backwards and will produce a false rib motion reading.
- Have your hands at the infrasternal angle.
- Get the patient to then take a normal breath in and out.
- Monitor the infrasternal angle during inhalation and exhalation.
Interpreting the Infrasternal Angle movement during breathing:
If ISA widens during inhalation, but does not narrow during exhalation — a person is known to be inclined or biased towards a wide angle.
If the ISA is biased or restricted in a narrow position —the infrasternal angle may not widen, instead the ribcage may roll backwards or elevate to initiate inhalation.
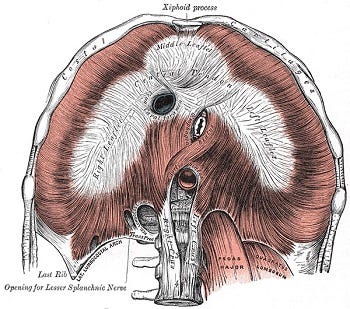
Consider the Diaphragm and it’s attachments:
Anterior fibres insert into the xiphoid process and travel alongside the costal margin.
Laterally the diaphragm inserts into ribs 6–12.
Posteriorly the diaphragm muscle fibres insert into T12 Vertebra and splits off into two appendages (Right and Left Crus).
The Right and Left Crus insert into the lumbar vertebrae.
Right Crus: L1–3 Intevertebral Discs
Left Crus: L1–2 Intervertebral Discs
As the angle widens or narrows — the diaphragm moves accordingly.
Ribs
Ribs 1–7 have a shared attachment at the sternum.
Ribs 1–7 are known to move as a cohesive unit
Ribs 8–12 do not share an attachment at the sternum instead converge at the costal cartilage and do not move as a cohesive unit.
What Constitutes Normal Mechanics?
- Infrasternal angle is Opposite to Infrapubic Angle
Properties of Inhalation:
During “Normal” Inhalation the following can be observed.
- Infrasternal Angle Widens (Inhalation)
- Diaphragm Descends > Drawing air into Thoracic Cavity
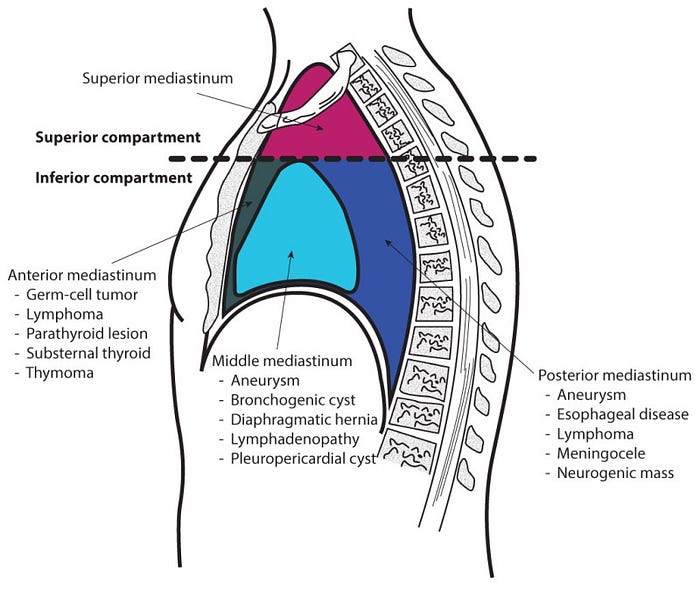
- Expansion/ Kyphosis of Posterior Mediastinum
- Ribs Bucket Handle Upwards
- Decrease in Lumbar Lordorsis
- Counter Nutation of Sacrum (Tilting Back of Sacrum Relative to Iliac Bones)
- Anterior Rotation of Pelvic Bones (Flexion Abduction, External Rotation) — NOT TO BE CONFUSED WITH ANTERIOR PELVIC TILT
How does this affect the spine & pelvis during other instances of Infrasternal Angles?
One Significance in Having a good Infrasternal Angle is during “Inhalation” The diaphragm is able to descend to create intrabdominal pressure that pushes the “Abdominal contents and guts” down into the pelvic inlet.
This creates an eccentric lengthening of the pelvic floor muscles.
A Wide Infrasternal Angle Bias/ Inclination (>90, 110–120deg)
- Increase in Thoracic Kyphosis
- Increase in Lumbar Lordorsis
- Nutation in Sacrum (Tilting of Sacrum Forwards relative to Pelvis)
A wide infrasternal angle would mean that the false ribs are in an “inhalation” position; causing the diaphragm to be overly “flat”. Similarly the Infrapelvic angle remains wide and the pelvic floor is flat which does not create room for the abdominal gut contents to descend.
An observable phenomenon would be the guts expanding outwards during inhalation/ big stomach and big kyphosis creating an imbalance.
A Narrow Infrasternal Angle Bias/ Inclination (<90deg)
- Decrease Thoracic Kyphosis
- Decrease Lumbar Lordorsis
- Counter Nutation in Sacrum
Having a narrow infrasternal angle would typically mean that an individual can achieve expansion at the front of the thorax but not expand the posterior part of the thorax. Scapula may be biased towards adduction/ closer to the midline of the spine/ poor Shoulder ROM.
When the ISA is too narrow (<90 deg) The diaphragm can be put into a difficult position where it can no longer move through regular ranges during breathing. The External Obliques can also end up over active and pull the ribs too close together.
A narrow infrapubic angle would also mean that the pelvic floor is overly lengthened, which doesn't create enough abdominal pressure.
Application of the Infrasternal angle
To be Continued….
Lee Won-hwee. Reliability and Validity of Measurement of Infrasternal Angle by Radiographic Methods. J Musculoskelet Sci Technol 2018;2(2):33–37.
